This study measures how effectively a treatment system can re-describe itself, not how meaningfully it changes for families.
On April 7, 2026, Catalight issued a press release announcing what it described as a shift in how families define “success” in autism treatment. The release states that parents no longer prioritize fixing their child’s behavior and instead value happiness, belonging, and wellbeing. The framing suggests a correction to decades of deficit-based care. It positions Catalight as the institution that has recognized and operationalized this change. The underlying study, however, does not establish a shift. It reports a qualitative analysis of caregiver responses at intake within a single service system.
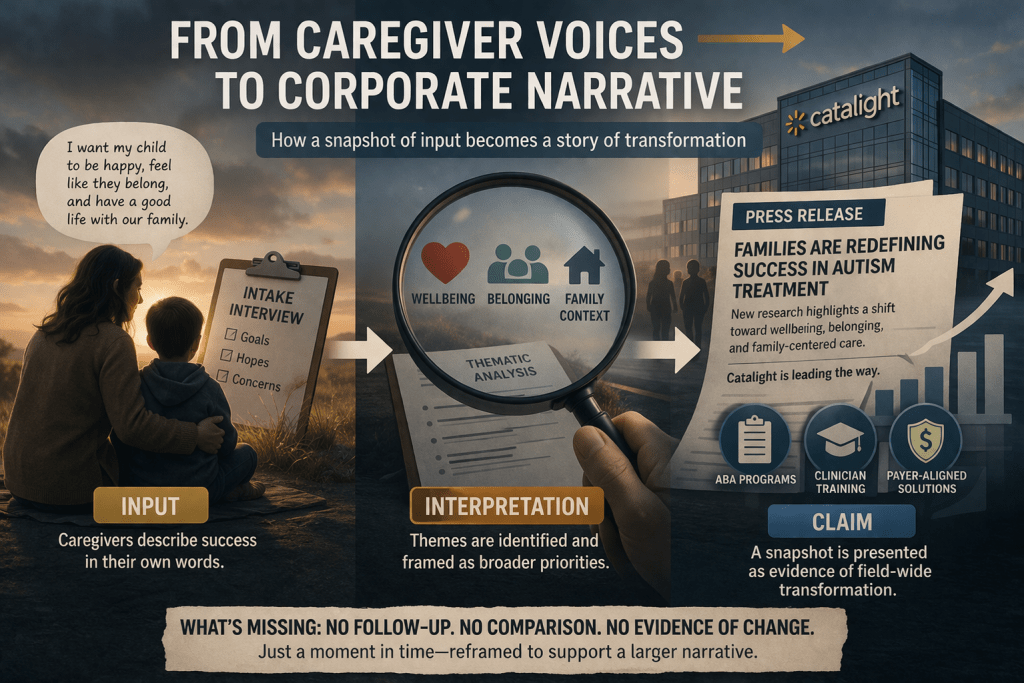
Caregiver language becomes evidence, and that evidence is then used to support institutional claims.
The difference between those two claims is structural. A shift requires comparison across time or populations. The study, as publicly available, presents neither. It examines 81 caregivers entering treatment for their autistic children, and identifies thematic patterns in how they describe success and barriers. Those responses include desires for emotional wellbeing, family support, and practical functioning.
These findings are consistent with longstanding parent reports across clinical and educational contexts, and are consistent with existing literature rather than demonstrating a novel shift. The Catalight study does not demonstrate that definitions of success have changed for autism families. They demonstrate that when caregivers are asked open-ended questions, they describe relational and practical concerns rather than technical behavioral targets.
The caregivers were asked these two questions:
- “What does success or graduation look like for the client or caregiver?”
- “Are there barriers to meeting these goals?”
Caregivers commonly describe success in terms of their child’s wellbeing and happiness. These responses reflect common caregiver priorities rather than a demonstrated shift in the field.
The research team represented disciplines including marriage and family therapy, mental health counseling, clinical psychology, behavior therapists, and nursing clinicians. The framework emphasizes both supporting the autistic child and empowering the family. The data were collected within a Catalight-affiliated service system operating through payer-funded care, while the study itself reports no external funding or conflicts of interest. The authors’ declared affiliations are within the Catalight organization rather than an independent research institution.
Beyond their closed-access “research” study, the press release expands those findings into a field-wide narrative. It states that “for decades” success has been measured through behavioral change and contrasts that with what families now want. This contrast is not tested within the study. It is asserted. The rhetorical move converts a bounded qualitative dataset into a broad communicative claim.
The structure of the study itself reinforces this pattern. The abstract describes a thematic analysis conducted at intake and concludes that caregiver perspectives challenge child-only models of care. It then moves to a second claim. It presents these findings as support for the suitability of Marriage and Family Therapists to lead autism treatment. The transition is immediate. Caregiver descriptions become justification for professional positioning. In anticipation of a federal ban of ABA billing codes, it is a logical preparation by an industry to speculatively justify billing under other clinical codes for “autism treatment”. This translation occurs within a specific institutional structure.
The study does not actually prove that Marriage and Family Therapists are needed in autism treatment. Instead, it takes what parents say at intake, organizes those answers into themes about family stress and support, and then uses those themes to argue that MFTs should lead care. Parents saying they are stressed, want help, and care about their family’s wellbeing is expected. That does not automatically mean a new type of therapist is required. The study never compares different types of care or shows that families do better with MFTs. It also does not look at whether adding more providers makes things harder, more expensive, or more complicated for families. Instead, it expands the idea of treatment to include the whole family, then presents MFTs as the solution to that expanded definition. In this way, parent concerns are turned into a reason to grow the system, rather than evidence that the system itself needs to change. The study claims MFTs should lead care without showing that children actually benefit from their involvement.
Catalight is not only a research entity. It is a service provider, a training platform, and a payer-aligned organization. It delivers treatment, trains clinicians, and produces outcome data. Within this configuration, research does not operate independently of service delivery. It circulates within it. The same system that defines treatment also evaluates and narrates it. The study’s conclusions therefore function within a context that benefits from demonstrating responsiveness to critique while maintaining continuity of service. A parent wanting their child to experience joy does not, on its own, indicate a shift away from behavior-based treatment.
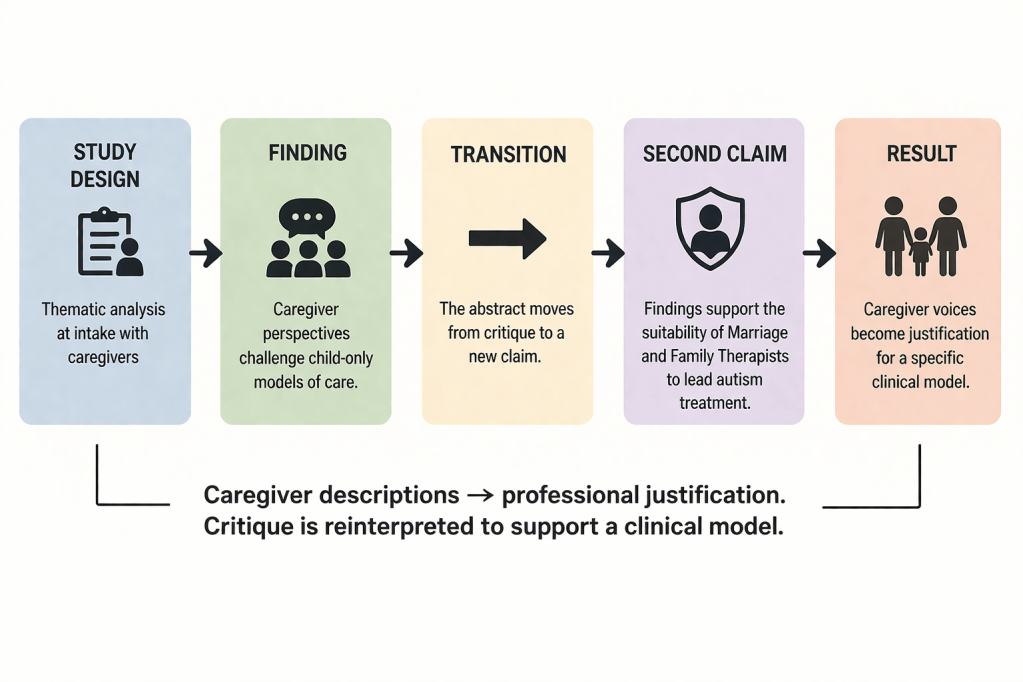
Flowchart showing how caregiver input is transformed into a professional claim through sequential interpretation steps.
The paywall intensifies this dynamic. The article is not publicly accessible in full. What can be examined without payment is limited to the abstract and metadata. The press release, by contrast, is fully open and widely distributed. The result is an asymmetry between narrative reach and evidentiary access. Readers encounter a broad claim about shifting definitions of success without the ability to review methodological detail, coding procedures, or limitations. The expansion of the claim cannot be easily checked against the full text.
This pattern aligns with earlier Catalight’s messaging. In January 2026, the organization highlighted research showing no clear benefit from increased ABA hours. The finding was framed as a question of intensity. The underlying framework of behaviorism remained unchanged. The focus shifted to dosage, defined as 20 to 40 hours of ABA per week, as the variable requiring adjustment.
The current release operates at a different level while maintaining the same structure. The endpoint is expanded rather than replaced. Behavior is no longer described as the sole outcome. Terms such as wellbeing, belonging, and family context are incorporated into the definition of success. These additions do not displace the existing model. The organization continues to offer ABA-based programs, clinician training, and payer-aligned solutions. The descriptive range of the system expands while its structure remains intact.
The introduction of family-centered language does not reorganize these arrangements. It overlays them. The language of critique becomes part of the service model.
What the study demonstrates, within the limits of its design, is straightforward. Caregivers entering treatment describe success in terms that extend beyond behavior reduction. This is an expected finding given the format of intake interviews and the lived realities of families. The press release assigns them a second function. It interprets those responses as evidence of a broader transformation in the field and positions Catalight as the institution aligned with that transformation.
This interpretive step introduces the misrepresentation. The study does not track change over time. It does not compare caregiver responses across periods or treatment models. It does not examine whether practices have shifted in response to these perspectives. It documents a set of responses at intake and extends them into a claim about systemic change.

Caregiver input is scaled into a story the data does not support.
The consequence extends beyond overstatement. The study is used to reclassify the system itself. A service model that has been the subject of critique is presented as the location of its resolution. The critique is translated into institutional language and returned as evidence of adaptation. The boundary between responding to criticism and incorporating it into branding becomes difficult to trace.
This dynamic does not require speculation about intent. It is visible in the alignment between study design, abstract conclusions, and press framing. A qualitative intake study is presented as evidence about the direction of the field. Caregiver language is used to support professional positioning. Limited access to the full article coincides with expansive public claims.
This pattern is familiar within behavior-analytic research contexts. Measurement remains precise at the level of procedure and expansive at the level of interpretation. The study documents how caregivers describe their goals. The press release translates those descriptions into evidence of institutional legitimacy.
This study exists to demonstrate alignment between caregiver language and Catalight’s service model, while ensuring that the underlying structure of ABA-based care remains intact. It documents continuity while presenting it as change.

Leave a comment