When ABA Defends Its Problem Behavior
In the wake of the Wall Street Journal investigation into the Medicaid autism therapy boom, some Applied Behavior Analysis (ABA) providers have adopted a new rhetorical posture: the insider-critic.
These are clinicians who acknowledge ethical problems in the ABA industry while simultaneously reaffirming their own authority to continue delivering the same model.
Heather Gonzales, Ph.D., BCBA-D, NPI #1669738878 exemplifies this phenomenon.
Her recent public commentary praises autistic-led investigations into Medicaid fraud and criticizes private-equity-driven ABA expansion. At first glance, this looks like a break from the status quo. But a closer examination of regulatory records and her own professional trajectory suggests something else:
ABA defending itself by defending the behaviorist.
How the Heather Gonzales case appeared in public records
The situation involving Arizona behavior analyst Heather Gonzales, Ph.D., BCBA-D first surfaced not through a public disciplinary action but through meeting minutes of the Arizona Board of Psychologist Examiners’ Committee on Behavior Analysts.
This is important because Arizona law intentionally limits what the public can see about complaints and investigations.
The public record therefore often appears indirectly, through meeting agendas and minutes rather than through the board’s official “disciplinary actions” database. The events described here are based on publicly available board records and statements; the analysis reflects a broader critique of systemic patterns rather than findings of wrongdoing beyond those records.
The regulatory moment behind the rhetoric
According to the January 9, 2026 Committee on Behavior Analysts meeting minutes, the board reviewed Gonzales’s license renewal application and discussed whether a complaint investigation should be opened.
The issue stemmed from a continuity-of-care problem involving a client at the agency she co-founded.
While Gonzales was away from the practice for approximately ten days, a non-licensed business partner discharged a high-needs adult client without notice or referral, creating a lapse in services that prompted a complaint from the Arizona Division of Developmental Disabilities.
The committee reviewed the situation as part of her license renewal and questioned whether her solo-licensee practice structure had sufficient contingency planning to protect vulnerable clients.
Her response is revealing.
Instead of disputing the event itself, Gonzales reframed the discussion around her own status as a disabled professional. She asserted rights under the Americans with Disabilities Act and characterized her emergency-coverage plan as a reasonable accommodation allowing her to remain a sole practitioner while continuing to supervise services.
After discussion and an executive session, the committee ultimately voted to:
- recommend approval of the license renewal
- not open a complaint investigation
- send Gonzales a formal letter recommending practice-management improvements
These recommendations included strengthening emergency coverage and continuity-of-care planning.
From a regulatory standpoint, the matter closed.
From a misbehaviorist standpoint, it illustrates a deeper pattern.
Unplanned Discharge. When oversight disappears, vulnerable clients can become administrative decisions—discharged without notice, without referral, and without continuity of care. For high-needs individuals, a gap in services is not just paperwork; it can mean immediate risk and systemic failure.
Regulatory Disclosure, Ethical Duties, and Public Protection
Arizona behavior analyst Heather L. Gonzales, Ph.D., BCBA-D, BHP disclosed during a licensing renewal process that she had been hospitalized for psychiatric reasons. According to statements attributed to her, the disclosure triggered a review by the Arizona Board of Psychologist Examiners, which oversees behavior analyst licensure in the state.
“Because I had to disclose to the psych board for my Arizona license renewal that I was hospitalized for psychiatric reasons. They are now having a hearing in which I could lose my license.”
LinkedIn post where Gonzales discloses the nature of her mental illness.
Professional licensing boards routinely review such disclosures because behavior analysts work with vulnerable populations, including autistic individuals and other disabled clients who may depend on providers for daily behavioral and safety support.
These reviews are part of a regulatory process designed to protect the public by ensuring clinicians remain mentally and professionally fit to provide services.
Arizona law also limits what information about complaints or investigations can be publicly disclosed. Under Arizona Revised Statutes §32-3214 and §32-2082, many complaints, investigations, and non-disciplinary actions do not appear on the board’s public disciplinary actions page. However, investigations themselves remain confidential unless formal disciplinary action is taken or records are released by court order.
Since the investigative file is confidential, the only place the public often sees evidence of a complaint review is in meeting minutes. When a licensing committee discusses a renewal application or complaint, the discussion is summarized in minutes that are posted publicly after the meeting. Those minutes can reveal:
- that a complaint occurred
- the general nature of the concern
- the committee’s decision
But they typically exclude detailed investigative information.
Where the public can find the board minutes
The Arizona Board of Psychologist Examiners publishes meeting minutes on its website. Readers can access them here: Arizona Board of Psychologist Examiners – Meeting Minutes. The relevant document is: Committee on Behavior Analysts Regular Session Minutes January 9, 2026.
Arizona law does allow members of the public to request additional records. Under A.R.S. § 32-3214(C), a person may request:
- dismissed complaints
- non-disciplinary actions
- disciplinary actions older than five years
These must be obtained through a public records request submitted to the board.
However, the investigative file itself remains confidential unless a court orders its release. The Gonzales review illustrates how regulatory oversight can exist without appearing in the public disciplinary database.
For members of the public trying to understand how behavior analysis clinics are regulated, this structure can make oversight appear invisible.
The oversight process may still occur, but it is often visible only through meeting minutes, renewal discussions, and public records requests, rather than through the board’s disciplinary actions page.
Ethical obligations under the BACB Code
Behavior analysts certified by the Behavior Analyst Certification Board (BACB) are required to follow the Ethics Code for Behavior Analysts, which establishes safeguards designed to protect vulnerable clients. Key ethical obligations include:
- Impairment self-reporting: Behavior analysts must disclose any medical or mental health condition that could impair their ability to deliver safe and effective services. If impairment could affect professional judgment or client safety, practitioners are expected to seek treatment, supervision, or temporary removal from direct service roles.
- Competence and professional fitness: BCBAs may only provide services within the limits of their professional competence and physical or mental capacity. If a condition could compromise service quality or client welfare, practitioners must take appropriate corrective steps.
- Protection of vulnerable clients: The BACB code emphasizes that behavior analysts must prioritize the safety, dignity, and rights of clients, particularly autistic individuals and others who may depend on behavioral support services.
- Mandated reporting: If impairment or misconduct creates risk of harm, supervisors or colleagues may have a legal and ethical obligation to report concerns to licensing boards or relevant authorities.
These safeguards exist to ensure that services provided to autistic and disabled individuals are safe, ethical, and professionally supervised.
The misbehaviorist inversion
Behaviorism traditionally frames clients as systems of observable behavior to be managed through environmental contingencies.
Misbehaviorism flips this framework onto the defense of the behaviorist herself. In this inversion:
- The client becomes peripheral to the narrative.
- The practitioner becomes the vulnerable subject.
- Structural concerns about the model are reframed as potential harms to the practitioner’s ability to practice.
The board discussion about continuity of care began as a question about client safety. By invoking disability rights, the focus shifted to the rights of the provider.
The contingencies of sympathy and attention were redirected. This is not an accusation of bad faith; it is a description of how behaviorist logic functions in institutional settings. Systems protect themselves by reorganizing narratives around the individuals who embody them.

Misbehaviorism. When scrutiny falls on the system, the narrative flips: the client fades into the background while the behaviorist becomes the vulnerable subject. Structural harms are reframed as threats to the practitioner’s ability to practice—shifting sympathy, attention, and accountability away from those the system claims to serve.
The “ethical insider” posture
Gonzales’s public messaging can be understood as aligning with this pattern. On social media she:
- criticizes private-equity-driven ABA expansion
- praises autistic researchers exposing Medicaid fraud
- acknowledges controversy surrounding early ABA research
But she does not challenge the foundational premise that ABA should continue as the dominant framework for autism services.
Instead, the message is:
The model is good.
The problem is bad actors or corrupted incentives.
This rhetorical move preserves the system while appearing reformist.
Heather Gonzales LinkedIn Posts — The “Ethical Insider.”
Publicly criticizing industry abuses while framing the crisis as a problem of bad actors and incentives rather than the behavioral model itself.
Boundaries, bait, and the politics of “dialogue”
For several years, I have maintained a clear public boundary:
I do not engage in discourse with behaviorists.
The reason is simple. Debate about whether behaviorism can be made more ethical often functions as a mechanism for rehabilitating the reputation of the system rather than examining whether the system itself should exist.
Despite that boundary, attempts at engagement continued. The pattern is familiar to many autistic critics of ABA: invitations to “talk,” requests for collaboration, appeals to shared values, and repeated efforts to draw critics into conversations framed as professional dialogue.
But dialogue is not neutral.
Within the ABA ecosystem, dialogue frequently serves a specific function: it absorbs critics into the reform narrative. Autistic researchers and whistleblowers become advisors, consultants, or symbolic validators of “trauma-informed” ABA, while the underlying structure of behavioral control remains intact.
My position has been consistent. I do not collaborate with systems whose foundational premise treats autistic people as subjects of behavioral modification.
Turning the lens toward the system
Instead of participating in that discourse cycle, the strategy has been to examine something regulators actually track: billing and service delivery.
Federal and state oversight bodies are not primarily concerned with philosophical debates about behaviorism. They focus on measurable issues such as:
- whether services billed to Medicaid were actually delivered
- whether supervision requirements were met
- whether continuity of care was maintained for vulnerable clients
These are operational questions about services rendered versus services billed.
When the behaviorist model claims to produce measurable outcomes, it implicitly invites this same level of measurement to be applied to its own operations.
In other words: if behavior analysts claim expertise in monitoring contingencies and compliance, regulators can reasonably expect those same standards of accountability from the clinics themselves.
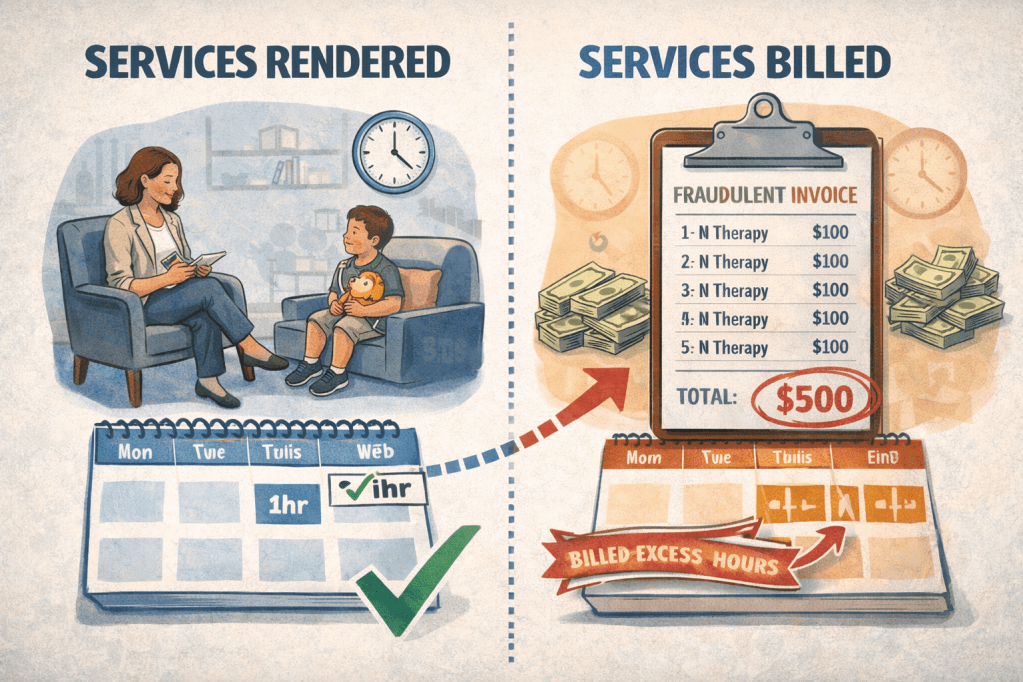
Services Rendered vs. Services Billed.
Regulatory oversight often comes down to a simple question: do the documented therapy hours match the services actually delivered? When billing exceeds care, the discrepancy becomes a matter of public accountability.
The accountability standard
If ABA positions itself as a health service funded by public programs, it enters a domain where scrutiny is unavoidable.
Regulators evaluate:
- continuity of care
- ethical billing practices
- supervision requirements
- discharge procedures
These are not ideological questions. They are administrative ones.
And once the system is evaluated on those terms, the conversation shifts away from debates about behaviorism’s theoretical foundations and toward something more concrete: whether the service infrastructure actually functions in the public interest.
That is where the current moment of scrutiny is focused.
Four children and a stopwatch
Gonzales’s doctoral research illustrates the epistemology underlying this system.
Her dissertation examined “motivation” in four disabled children using a single-subject design. Participants performed simple tasks (such as matching picture cards) in exchange for reinforcers like snacks or brief cartoon clips.
Motivation was operationalized entirely in behavioral metrics:
- latency to respond
- task duration
- percent correct responses
- number of non-responses
Notably, the results showed undifferentiated data, meaning the experimental conditions produced no clear differences. Yet the study was still framed as contributing to the ABA evidence base.
This pattern is common in behavior analysis: procedural rigor substitutes for conceptual depth. If behaviors are defined, measured, and graphed correctly, the work counts as science, even if the phenomenon under investigation remains poorly understood.
The stopwatch becomes evidence.
The complex-case niche
After credentialing, Gonzales built a practice focusing on autistic and intellectually disabled teens and adults with severe behavioral challenges.
This is a population frequently described by ABA providers as “underserved” because many clinics concentrate on younger children.
But the niche also intersects with a key economic reality.
Complex clients often qualify for intensive Medicaid-funded services, particularly when their behaviors are framed as safety risks involving hospitalization, law enforcement, or property destruction.
In this context, behavior plans function simultaneously as:
- treatment protocols
- risk management tools
- reimbursement justifications
The same behavioral data that structures treatment can also sustain billing streams.
The structural incentive problem
ABA’s rapid expansion over the past decade has been fueled by a particular economic arrangement: insurance and Medicaid reimbursement tied to hourly behavioral services.
That structure creates incentives for:
- high-intensity treatment hours
- large technician workforces supervised by relatively few clinicians
- clinic ownership models that scale rapidly as demand grows
For many practitioners, obtaining advanced credentials and clinic ownership status is framed as a professional achievement. But the financial structure also creates a system where continued expansion is necessary to sustain the business model.
Critics describe this as an incentive loop: training programs produce more certified practitioners, those practitioners open or manage clinics, and the system expands to absorb the workforce it produces.
The question for regulators is not whether individual practitioners have good intentions. The question is whether the structure reliably produces safe, accountable services for vulnerable clients.
Grooming critics into consultation
Another feature of the insider-critic posture is the recruitment of critics themselves.
When ABA clinicians publicly praise autistic researchers who expose industry abuses, a subtle dynamic emerges:
Critics are invited to help refine the system.
They are asked to consult on:
- ethical frameworks
- trauma-informed approaches
- regulatory reforms
- improved treatment plans
The fundamental question, whether the behaviorist model should dominate autism services at all, remains outside the discussion.
Criticism becomes quality-improvement labor.
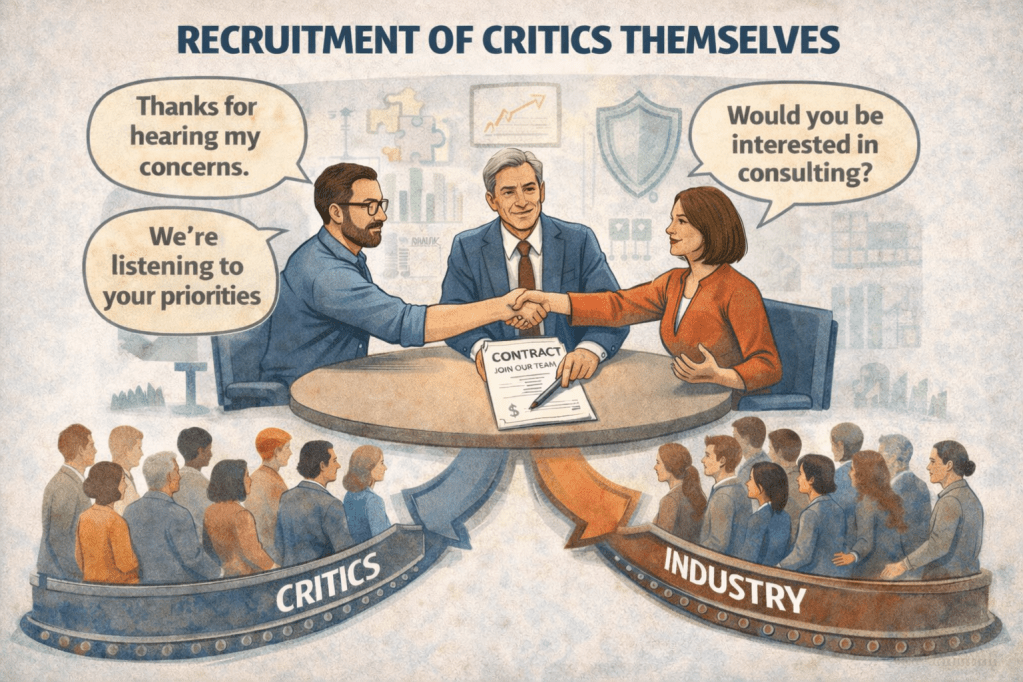
Recruiting the Critics.
When systems face scrutiny, critics are often invited inside—offered consultation, collaboration, and reform roles. The result can transform opposition into partnership, softening critique while leaving the underlying structure intact.
Why this matters now?
Recent investigations into the autism therapy industry have complicated the field’s long-standing effort to present Applied Behavior Analysis as a neutral, evidence-driven science. For years, the discipline relied on a narrative of clinical objectivity: ABA was framed as a technical intervention, guided by data and insulated from ideological dispute. That framing becomes harder to sustain when journalists, autistic researchers, and public agencies begin documenting structural problems within the industry itself; problems that include aggressive expansion, questionable billing practices, and the routine treatment of autistic behavior as a site of commercial service delivery.
In this new environment, outright denial of harm is increasingly untenable. The more effective institutional response has been a shift in narrative, from defense to reform. Rather than rejecting criticism, some practitioners now publicly acknowledge parts of it. They condemn private-equity consolidation of clinics, recognize the troubling history of early behavioral research, and amplify the work of autistic investigators who expose fraud within the Medicaid system. These gestures signal awareness and empathy. They position the speaker as someone who understands the concerns being raised.
Yet this rhetorical move rarely challenges the foundational premise of the system itself. The dominant message is not that the behavioral model should be reconsidered or displaced, but that it has been distorted by bad actors and corrupted incentives. In this framing, ABA remains fundamentally sound; the problem lies in how the industry surrounding it has been managed. Reform becomes the solution, more oversight, more ethics training, better billing controls, while the central authority of the behavior analyst remains intact.
Figures like Heather Gonzales illustrate how this posture functions within the broader ecosystem of professional legitimacy. By acknowledging controversy and aligning themselves with calls for accountability, such practitioners present themselves as ethical insiders: clinicians who are capable of guiding the field through its current crisis without abandoning its core assumptions. The stance carries both moral credibility and institutional continuity. It allows the profession to absorb criticism without fundamentally restructuring the system that produced it.
The concept of misbehaviorism helps explain why this strategy is effective. When institutions face sustained scrutiny, they rarely defend abstract doctrines or theoretical frameworks. Those are difficult to humanize, and even more difficult to protect rhetorically. Instead, institutions defend the individuals who embody them. The debate shifts away from structural questions; how the system operates, whom it benefits, and whether it should exist in its current form, and toward the personal circumstances, intentions, and vulnerabilities of the practitioners themselves.
In that inversion, the behaviorist becomes the sympathetic figure. Discussions that begin with the welfare of autistic clients or the ethics of behavioral control gradually reorganize around the challenges faced by clinicians: the pressures of regulation, the burdens of oversight, the emotional strain of working in a controversial field. Once attention centers on the practitioner rather than the structure, the terms of the conversation change. Criticism appears less like systemic analysis and more like a potential threat to the livelihood of a particular professional.
This is the moment where misbehaviorism reveals its central mechanism. By defending the behaviorist, the institution effectively defends itself. The individual practitioner becomes the visible stand-in for the larger framework of behavioral authority. Sympathy for the person translates into tolerance for the system they represent.
And once that shift occurs, once the behaviorist is understood primarily as a vulnerable actor navigating a flawed but necessary profession, the structural critique loses its leverage. The model itself remains in place, the authority of the practitioner remains intact, and the broader system continues to operate largely unchanged.
While these elements are not unique to a single case, they illustrate how individual incidents can reflect broader structural dynamics within the industry.
Sympathy as Strategy.
When criticism targets a system, attention can shift toward the practitioner who represents it. Sympathy for the behaviorist reframes structural questions as personal struggles, softening scrutiny while the underlying system remains intact.

Leave a comment